Dallas
214-456-2240
Fax: 214-456-8881
Plano
469-497-2501
Fax: 469-497-2507
Request an Appointment with codes: Plastics and Craniofacial Surgery
214-456-2240
Fax: 214-456-8881
469-497-2501
Fax: 469-497-2507
Request an Appointment with codes: Plastics and Craniofacial Surgery
Unilateral coronal craniosynostosis causes about 15% of all isolated craniosynostosis cases. Unlike sagittal and metopic suture craniosynostosis where the changes in the head shape are symmetric, closure of one coronal suture creates a significant uneven appearance to the skull and face.
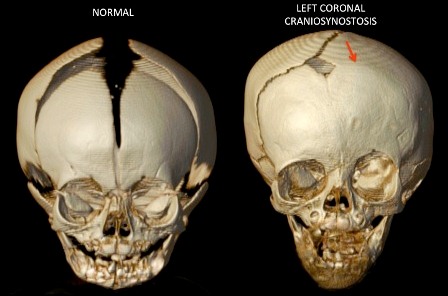
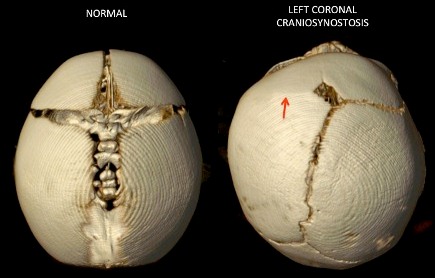
These patients have flat foreheads and raised eye sockets on the side of the closed coronal suture. On the side with the open coronal suture, their forehead is fuller and the eye socket is vertically shorter. This uneven appearance is the result of constricted growth on one side and compensatory growth on the other.
The role of strip craniectomy and using a postoperative helmet in these patients is not yet clear, although we do occasionally offer this on a case-by-case basis. The mainstay of treatment in these patients has been an open cranial vault remodeling with a fronto-orbital advancement. This allows the surgeon to over correct the closed side and reshape the eye socket to allow the patient to “grow into” the correction.
There has been greater interest in using extended strip craniectomy with post-operative helmeting in these patients. We feel that this approach will often undercorrect the abnormal contour of the eye socket and forehead when compared to the degree of improvement seen in open cranial vault procedures. We still use this approach, though not as frequently.
For the majority of our patients we use fronto-orbital advancement to increase the volume inside the skull and overcorrect the position of the forehead and eye socket, placing these bones as far forward as possible. The goal is to overcorrect the position of the forehead and eye socket as much as possible because the bones will not move forward because of the closed coronal suture. So we overcorrect and allow the child to grow into the correction so they will achieve a normal skull shape as they approach completion of the skulls growth which is over 90% grown by age 5.