Dallas
214-456-2240
Fax: 214-456-8881
Plano
469-497-2501
Fax: 469-497-2507
Request an Appointment with codes: Plastics and Craniofacial Surgery
214-456-2240
Fax: 214-456-8881
469-497-2501
Fax: 469-497-2507
Request an Appointment with codes: Plastics and Craniofacial Surgery
Isolated craniosynostosis, also known as non-syndromic craniosynostosis, is the most common type of craniosynostosis and occurs when one suture in the skull closes. The six major skull sutures affected are the metopic, the two coronal sutures, the sagittal suture, and the two lambdoid sutures. Babies with isolated craniosynostosis usually do not have other health problems at birth.
A different and rare form, called syndromic craniosynostosis, is caused by one or more sutures closing too soon. These babies are also born with other medical problems. Syndromic craniosynostosis is treated very differently from isolated (non-syndromic) craniosynostosis.
The types of isolated craniosynostosis are:
Isolated craniosynostosis occurs in about one in 2,500 births. The most common type is closure of the sagittal suture. This makes up about half of all cases.The metopic suture is the only cranial suture that normally closes before adulthood. It usually closes at about 8 months of age. All remaining sutures should remain open until adulthood, long after the brain has stopped growing.
The two biggest concerns related to craniosynostosis are:
Very high pressure in the skull can cause learning delays and blindness. There is a 15% risk for increased pressure developing in the skull when a single suture is closed.
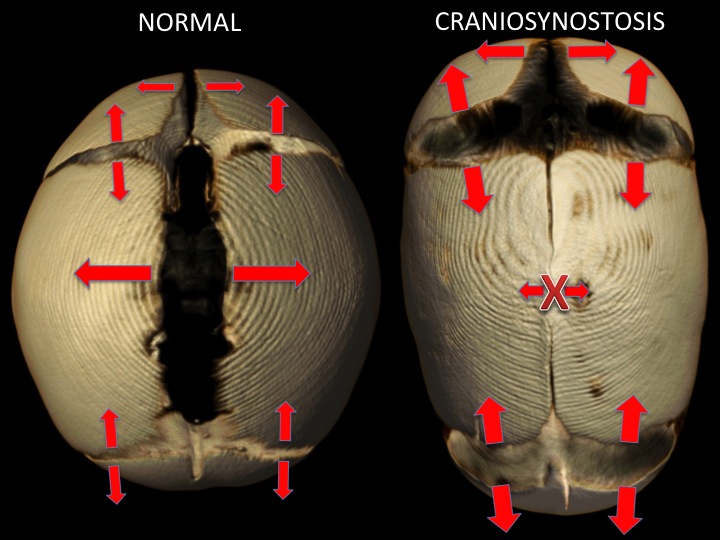
Almost all of the growth of the skull bones occurs at the cranial sutures. The cranial sutures are the seams or indentations visible in the skull. These serve as growth centers for the skull bones similar to the growth plates in the long bones. The growth occurs perpendicular to (away) from the suture. The growth of the brain below the skull bones is what drives the growth of the skull. The growing brain “stretches” the sutures which stimulates them to create bone to make room for the enlarging brain. This system allows the skull to remain just large enough for the brain it protects. The shape of the skull is in many ways controlled by the shape of the brain. If a suture closes earlier than it is designed to (before growth of the brain and skull is complete) it is called craniosynostosis. The only suture that is designed to close during infancy is the metopic/frontal suture. When a suture closes earlier than it should the skull bones in the area of the suture can’t grow. This is a problem because the brain continues to grow at the same pace so the remaining open sutures must make up the difference and grow more bone to create enough space for the growing brain. Closure of each of the major sutures causes a recognizable pattern of growth and abnormal head shape. The position of the closed and remaining open sutures determines how the skull will grow and what the shape will be.
Some kind of surgery is needed to treat isolated craniosynostosis. Most patients with single suture craniosynostosis do not develop increased pressure on the brain in the first year of life. There are few urgent reasons to operate during the first year of life. However, the timing and scope of the surgery depend on:
For reshaping the skull, it is best to perform surgery before 1 year of age. This is best because:
The goal of treatment is to balance the remaining growth at the open sutures with the lack of growth at the closed suture(s) to achieve as normal a head shape as possible. This usually requires an overcorrection of the head shape that the patient grows into over time. We use many different surgeries and other treatments to achieve these goals. Different procedures may be recommended for patients with the same suture affected.
We base our recommendation for the type of procedure based on what is safest for the patient while providing optimal results in function and appearance. At Children’s Health℠ we use several of the newer surgeries for skull reshaping such as:
We also use traditional open cranial vault procedures such as:
The types of surgery we use depend on what suture is closed. Early diagnosis of elevated pressure inside the skull can prevent partial or total blindness and learning delays. This makes the diagnosis and prevention of elevated pressure in the skull our priority as we treat patients with craniosynostosis.
A team of many experts will examine your child to determine what treatment we will recommend. Each patient is seen by a plastic surgeon who specializes in reconstruction of the skull and face (craniofacial), pediatric brain surgeon (neurosurgeon) and a pediatric eye doctor (ophthalmologist).
We use head imaging scans such as CT and MRI, to view a baby’s skull to create a surgical plan. We also examine a baby’s eyes to watch for signs of pressure on the brain and eye problems.
We also can directly monitor the pressure inside the skull. This remains the most reliable tool for measuring the pressure, but it requires admission to the hospital. It also requires us to place a device inside the patient’s skull. So, we use this only for patients we suspect have increased pressure but are not sure that surgery is indicated, which is rare. Unfortunately, there are no reliable ways to use scans (radiology) to find increased pressure on the brain. A yearly eye exam is given to patients without symptoms of pressure. This tests looks for bulging of the optic disc at the back of the eye, which may be present if there is increased pressure inside the skull.


