Dallas
214-456-2240 Fax: 214-456-8881
Plano
469-497-2501 Fax: 469-497-2507
Request an Appointment with codes: Plastics and Craniofacial Surgery
214-456-2240 Fax: 214-456-8881
469-497-2501 Fax: 469-497-2507
Request an Appointment with codes: Plastics and Craniofacial Surgery
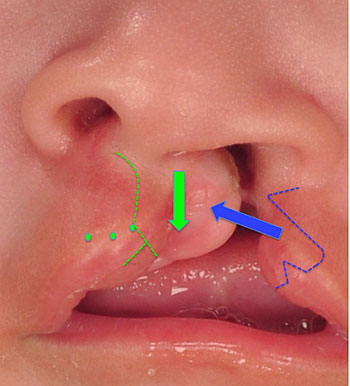
The goals of cleft lip repair are to close the skin, muscle and oral side of the lip and close the nasal floor while returning symmetry to the lip and nose. Incisions have to be made in order to achieve these goals.
Ideally, we can place our incisions where there are normal features of the lip, which allows us to disguise the resulting scars. This is most valuable in the vertical incisions we need to make that are disguised in the philtral column.
The patterns of repair for unilateral and bilateral cleft lip are tailored to the abnormal shape of the lip and nose and are shown below. Typically, the lip repair is performed in a single stage after nasoalveolar molding (NAM) is complete at approximately 3 to 4 months of age.
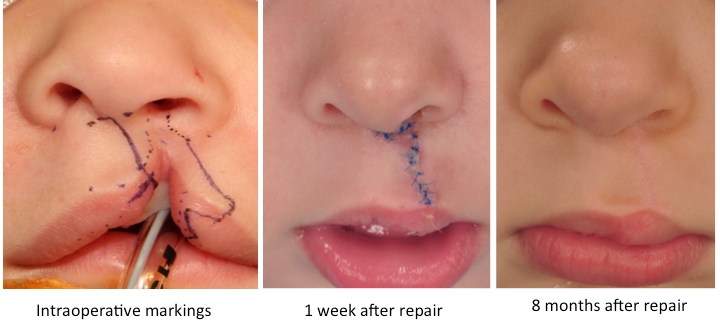
The goals of unilateral cleft lip are to rotate the middle portion of the lip down to level the Cupid’s bow of the lip and a nasal repair to restore symmetry to the nasal shape. See before and after photos.
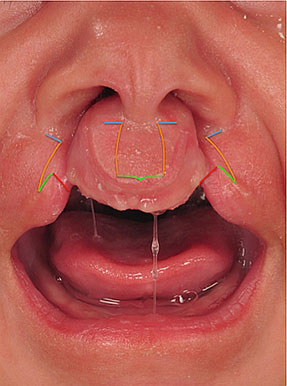
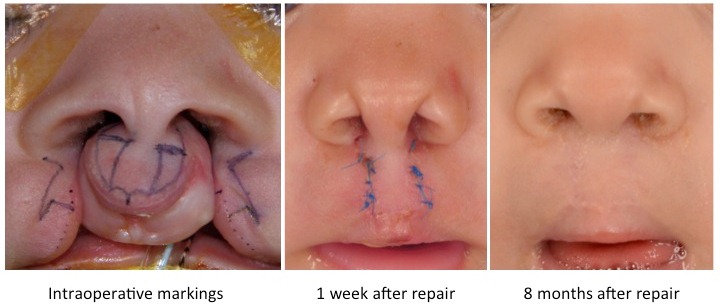
The goals of bilateral cleft lip are to bring the lateral parts of the lip together with the middle part of the lip to close the lip and create the missing philtral columns and create a Cupid’s bow. The nasal repair narrows the nose, restores symmetry to the nasal shape and lengthens the columella. See before and after photos.
Occasionally, a minor revision surgery of the lip may be needed later in childhood, but major revisions of the lip are rare. It is much more difficult to achieve a durable reshaping of the nose. The initial reconstruction of the nose provides a significant improvement in appearance but also creates scar tissue.
The nose goes through a rapid growth phase during puberty, which tends to bring out the original asymmetry because the scar tissue created by the original repair restricts growth in the area of the original repair of the nose. A rhinoplasty is commonly performed to address asymmetry when the patient is fully grown.
An important message for parents to understand is that children with cleft lip and palate require specialized care by a cleft team from the time of their birth until they are fully grown. The abnormal anatomy of the lip, nose and palate that results from both the original changes from the cleft and the scar tissue created by surgical repairs will have long-lasting effects on the growth of the face. Excellent long-term functional and aesthetic results are the product of a well-coordinated treatment plan through collaboration of all members of the team.
Here is the typical sequence and timing of potential surgeries needed for patients with cleft lip and palate:
Children born with cleft lip and palate are often missing gum tissue where they have cleft lip and palate. They are likely to develop malocclusion such as an underbite or crossbite. These malocclusions should be repaired before alveolar bone grafting surgery. The most common treatments are:

